Diagnostic Testing: Urinary Bladder Pressure
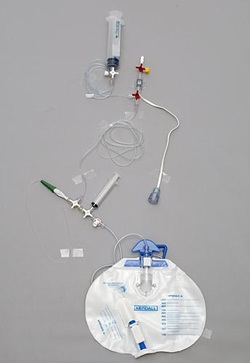 Image Source: The Royal Children's Hospital Melbourne
Image Source: The Royal Children's Hospital Melbourne
- Presence of sustained, elevated intra-abdominal pressure is the definitive diagnostic criteria for abdominal compartment syndrome (ACS).
- Urinary bladder pressure is an accurate proxy to measure intra-abdominal pressure and can be done in two ways:
- Place patient in supine position, insert Foley catheter, empty bladder, clamp off and then inject 25 to 50 mL of sterile saline solution; keep patient supine, use symphysis pubis as zero reference point, attach transducer to sampling port of Foley and measure readings on electronic monitor.
- Alternatively, instead of connecting a transducer to the Foley, raise Foley tubing above symphysis pubis at 90 degree angle, unclamp tubing and measure distance in cm between symphysis pubis zero point and maximum ht. of fluid in column. 1 cm = 1 mm Hg. Normal pressure in abdominal cavity should equal or be slightly below atmospheric pressure (< 0 ).
- Intra-abdominal pressures are classified as mild (10-20 mm Hg), moderate (20 - 40 mm Hg), severe ( > 40 mm Hg). However, decompression is usually done when pressures approach 30 mm Hg.
- Place patient in supine position, insert Foley catheter, empty bladder, clamp off and then inject 25 to 50 mL of sterile saline solution; keep patient supine, use symphysis pubis as zero reference point, attach transducer to sampling port of Foley and measure readings on electronic monitor.
Source:
Walker, J., & Criddle, L. M. (2003). Pathophysiology and management of abdominal compartment syndrome. [Review]. Am J Crit Care, 12(4),
367-371; quiz 372-363.
Walker, J., & Criddle, L. M. (2003). Pathophysiology and management of abdominal compartment syndrome. [Review]. Am J Crit Care, 12(4),
367-371; quiz 372-363.
